Symptoms.—Incubation period usually lasts from two to seven days after exposure, usually two, generally there is chilliness, sometimes convulsions in young children, pain in the back and extremities and a fever of 102-1/2 to 104 degrees.
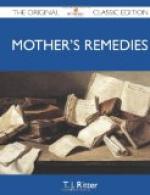
Pharyngeal diphtheria.—In typical cases this begins with slight difficulty in swallowing, and reddened throat (pharynx), then there is a general congestion of these parts, and membrane is seen on the tonsils. It is grayish white, then dull or yellowish; adherent and when removed it leaves a bleeding surface upon which a fresh membrane quickly forms. If the disease runs on, in a few days the membrane covers the tonsils and pillars of the fauces, often the uvula. The glands around the neck often enlarge. Temperature 102 to 103 degrees. Pulse 100 to 120. The constitutional symptoms are usually in proportion to the local condition, but not always. The membrane frequently extends into the nostrils and frequently there is a burning discharge. In malignant cases all the symptoms are severe and rapidly progressive ending in stupor and death in three to five days. Death may occur from sudden heart failure or complications.
[Infectious diseases 185]
[Illustration: Diphtheria (view of infected throat)]
Laryngeal diphtheria, Formerly Called Membranous Croup.—Diphtheria in the larynx may occur alone or with the pharyngeal kind, and was formerly called “Membranous Croup.” After several days of hoarseness and coughing the breathing suddenly becomes hard, generally at night, and it is at first in paroxysms, but later it is constant. The space above the breast bone (sternum) is depressed and there is a drawing in of the spaces between the ribs during inspiration accompanied with a husky voice and blue look. The fever is slight. If the obstruction in the larynx is severe the cyanosis,—blueness,—and difficulty of breathing increase, and gradual suffocation leads to (coma) deep sleep and death.
Diagnosis.—Diagnosis can only be made certain by proper chemical tests. The presence of membrane on a tonsil and a small patch streak, or speck of membrane, on the adjacent surface of the uvula or tip of the uvula; a patch of membrane on the tonsil and an accompanying patch on the posterior wall of the pharynx; the presence of a croupy cough and harsh breathing with small patches of membrane on the tonsil or epiglottis. These symptoms are very suspicious and warrant separation of the patient. If such conditions are seen in any one, it will be the part of prudence to send for your doctor immediately. You give the patient a better chance by sending early, protect yourselves and also your neighbors.
Recovery.—Chances in mild cases are good. Antitoxin has brought the death rate down from forty to twelve per cent. Death may occur from sudden heart failure, obstruction in the pharynx, severe infection, complications or paralysis.





